A Doctor’s View From the Front Line of the Omicron Wave

Alex Harding, MD. Entrepreneur in Residence, Atlas Venture; internal medicine physician, MGH
My phone buzzed with alerts about record-setting case numbers as I rushed between patients. A pile of tiny bottles with swabs floating in pink liquid accumulated while awaiting PCR testing.
Patients with coughs and sniffles lined up outside the door, waiting to be seen.
My shift as an internal medicine physician yesterday in MGH Chelsea’s urgent care facility reminded me of the early days of the pandemic.
The first wave was scary. The disease moved so fast. It was so severe. We knew so little.
We are certainly in a much better place this time around. But in terms of the raw numbers of people affected, the current wave is even worse.
On Monday, two days after Christmas, my clinic set a record for the number of patients seen. Shockingly, the rate of positive COVID tests has been 60-70% this week. That’s higher than I ever remember from the first wave. I tried to avoid eye contact with the people in the packed waiting area, as many patients waited over 3 hours to be seen.
It’s daunting as a healthcare worker to see this many people in line with COVID. But the feeling on the ground is different. Thanks to the vaccines and our familiarity with the disease, the illness severity is far less than before. We are seeing more patients with non-respiratory illnesses now than we saw in the first wave. And, after nearly two relentless years of pandemic pressure, fatigue has clearly set in among both healthcare workers and patients.
First, some numbers: I saw 19 patients during my 8-hour shift yesterday—about 3 or 4 more than I’d be able to get through in a busy shift before COVID. Of these patients, 11 had respiratory symptoms and 8 had other issues.
Remarkably, 10 of the 11 with respiratory symptoms had previously been vaccinated for COVID—6 had received 2 doses and 4 had received 3 doses. Only one of my respiratory patients, a young person who had very recently emigrated from Central America, was unvaccinated. Four of the patients I saw tested positive for COVID, below average for what my clinic has seen over the past week. These patients were mostly in their 20s to 40s, but in our clinic we are seeing patients with COVID spanning a full spectrum from infants to the elderly, with and without comorbidities.
Vaccines make all the difference
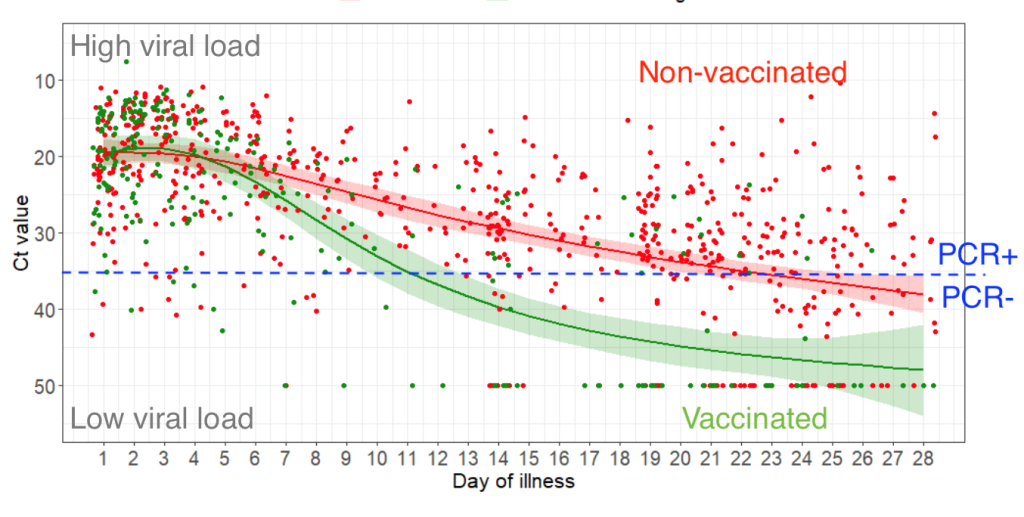
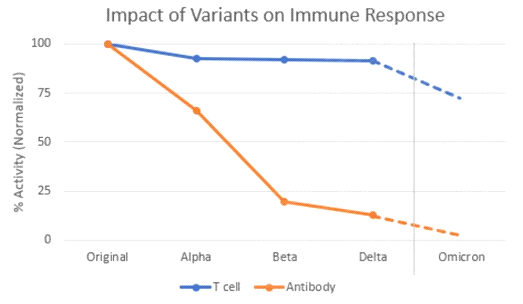
Of all the differences during this wave compared with prior COVID waves, the vaccination rate is the most important. The fact that all but one of my respiratory patients yesterday were vaccinated is both good and bad. This reflects the ability of the Omicron variant to at least partially escape immunity built up from prior rounds of vaccination or infection. That’s the bad news.
Now for the good news – these vaccinated patients with COVID had mild respiratory symptoms. They are not getting so sick that they develop Acute Respiratory Distress Syndrome (ARDS) — the kind of serious illness that requires mechanical ventilators.
Here’s what I mean by mildly ill. Almost all 11 of these patients had cold symptoms – runny nose, stuffy nose, sore throat, fatigue — but no shortness of breath. Only one patient, who was vaccinated, was slightly short of breath. None of my patients needed to be referred to the emergency department. They all went home.
The story was different in the first wave. There were days when we sent every third patient by ambulance to the emergency room—in March and April 2020, MGH had contracted with an ambulance company to keep an ambulance waiting at all times outside our front door.
Chelsea is an impoverished community of about 40,000 people, just across the Mystic River from Boston. The people who live here are mostly immigrants from Latin America. They do a lot of low-wage jobs and have limited access to healthcare. Despite these challenges, Chelsea has a vaccination rate substantially higher than the state average—an accomplishment featured in October in the Boston Globe.
Now, during the Omicron surge, it appears Chelsea is reaping the rewards. Its residents are mostly protected from severe illness and death from COVID.
The prevalence of vaccination completely changes how I take care of each patient. The patients I am seeing are uncomfortable, with stuffy nose and sore throat. But their vital signs are usually stable. They are not struggling for air.
My risk assessment for these patients’ progression is also dramatically different. In the past, I was unable to speculate about whether a patient was likely to turn the corner soon or whether the illness would worsen. Now, I can reassure the vast majority of patients that, thanks to the vaccine, their illness is unlikely to get much worse. Usually, this means they can go home, get some rest, drink plenty of fluids, and stay away from other people until they are no longer infectious.
There are people out there disparaging the vaccines, wondering why anyone should bother if they can be vaccinated and still get sick. But the vaccines are clearly getting the job done. They are keeping people out of the ER and the ICU and the funeral home.
We know what we’re doing now
Our familiarity with COVID and how to manage its effects has progressed dramatically. In the spring of 2020, aside from a few case reports from China and Italy, we were almost flying blind. We did not know precisely how the illness was spread, who was at highest risk, and how to treat patients who were sick.
The CDC told us we did not need to wear N95 masks when seeing COVID patients (we should have). We debated whether to keep patients in negative pressure rooms (probably overkill). We worried too much about fomites—passing the virus through direct contact—and not enough about airborne aerosol spread. Protective equipment was scarce and an enormous source of anxiety for many healthcare workers.
For months, we were forced to sift through a flood of weak evidence and inference to determine how best to treat patients. For a while, ibuprofen was strictly avoided and atorvastatin and hydroxychloroquine were the mainstays of therapy (wrong on all counts).
Today, while access to outpatient treatments is still severely limited, as I’ll discuss later, we have greatly improved inpatient treatment protocols with a combination of prone positioning, tailored oxygen therapy, dexamethasone, remdesivir, and prophylactic anticoagulation. If I ever have to admit a patient to the hospital, I feel confident that they will receive care that improves their chances of recovery.
It’s not just COVID anymore
Early on, while COVID cases shot up, patients with non-COVID conditions seemed to vanish. Of course, they did not truly go away; they just stayed home, which put them at risk of deterioration without proper medical care.
That has changed. While I saw 11 respiratory patients yesterday, I also saw 8 patients without respiratory issues. I saw a patient with substance use disorder, one with a nasty nosebleed, patients with urinary infections, gastrointestinal issues, and more.
Our clinic is not just dealing with the current COVID wave. We’re dealing with our usual steady flow of sick people, plus a COVID wave on top. This makes our days busier. In the bigger picture, though, it is a relief that our patients with non-respiratory issues are getting the help they need. As long as hospitals aren’t overwhelmed with COVID patients, this will remain true.
We’re all pretty tired
It’s been almost two years of this. It feels longer. It’s natural for us all to be tired. Healthcare workers have had a particularly difficult couple of years, having seen so many sick people with so little that we could do for them. We have put our own health on the line, especially in the days before the vaccines. Some of us feel that our employers haven’t fairly recognized that sacrifice. Many healthcare organizations have experienced a higher rate of turnover than usual. That has compounded the fatigue for the people who have stayed put and had to pick up the slack.
Scared as we all were in the early days, I was exhilarated by being able to help on the front lines.
I still look forward to my clinical shifts, but my level of excitement has moderated over time.
The fatigue is not just among the healthcare workers. Our patients are also tired. Yesterday, I saw some patients who seemed nonchalant about possibly having COVID. In part, this makes sense. For low-risk, vaccinated people, COVID infection is very unlikely to be severe. But being infected with COVID still warrants more than a shrug.
There is also increasing fatalism. It’s understandable that some people would question why they should bother adhering to public health recommendations when they still have not been able to avoid getting infected. That attitude was palpable in some of my patients.
In spite of the frustrating circumstances, it is important to weigh the risks and benefits of one’s actions. For most healthy, vaccinated people, it probably doesn’t make sense to go back to a full lockdown. But it also doesn’t make sense to throw caution to the wind by abandoning masks and basic precautions.
Some things haven’t changed
We still have very few treatments to offer outpatients with COVID.
With Omicron, we took a big step back in our therapeutic options for outpatients. The monoclonal antibodies from Regeneron and Eli Lilly were helpful against earlier variants, but don’t work against the new variant. There have been important treatments authorized by the FDA in recent weeks. But availability is limited.
Here’s the latest status for therapeutic options at my hospital:
- Sotrovimab – This is the only broadly neutralizing monoclonal antibody available for COVID at MGH. Because of extreme scarcity, it is only being given to the highest risk patients, those who are unvaccinated and have multiple risk factors. Even among those patients, only a fraction are chosen at random to get treated.
- (Aside: You should be uncomfortable with the concept of ‘penalizing’ people who have been vaccinated by not making this treatment available to them, but as physicians we must allocate resources to those who will most benefit and must not pass judgment against our patients based on the decisions they have made previously or the life conditions that influenced their ability to get the vaccine. Painful as it is, this is the right policy.)
- Paxlovid – MGH is expecting to receive about 100 courses of this new oral protease inhibitor medication in the next few days. This treatment will also be restricted to the highest risk patients, similar to sotrovimab.
- Molnupiravir – This drug, an oral polymerase inhibitor, will become available soon, and MGH is expecting to receive many more courses than it will receive of Paxlovid. However, thanks to the risk of inducing mutagenesis, it will probably be restricted to the highest risk patients who are not able to receive either sotrovimab or Paxlovid.
- Fluvoxamine – This drug, an old selective serotonin reuptake inhibitor sometimes prescribed for depression and obsessive-compulsive disorder, is not authorized for COVID. There is some clinical data supporting its efficacy against COVID. The mechanism of action is dubious and most doctors will be reluctant to prescribe it off label. For more, see The Lancet Global Health.
- Evusheld – This long-acting antibody cocktail was authorized early this month by the FDA for immunocompromised individuals. It can be used for prophylaxis, and it’s been shown to last 6 months. But it is not yet widely available to hospitals.
Over the next month or two, access to sotrovimab, Paxlovid, and Evusheld will hopefully improve and make a significant dent in COVID. For now, your best bet is to get a vaccine booster and wear a high-quality mask.
Public health still gets politicized
I was naïve enough to think that under Biden the CDC would regain scientific independence, but unfortunately that does not seem to have happened, at least not to the extent I had hoped.
Earlier this week, the CDC, with no data to support the decision, shortened the duration of quarantine for COVID patients from 10 days to 5 days. This news was a hot topic of conversation on the front lines. I spoke with about half a dozen patients yesterday about the CDC’s announcement. Some were uncomfortable with the change, and others were happy that they would be able to return to work sooner. In all cases, I had to discuss what the data actually show. (My advice to those patients: test before ending quarantine if possible, shorter quarantine for vaccinated than unvaccinated, and in no case less than 7 days.)
We’ll get through this
In spite of these challenges, I am confident that we are in a good position to get through this wave. Most of us are vaccinated and strongly protected against severe illness. For those who do get sick, we know how to take care of them. Hopefully, we will soon have new treatments available that will dramatically protect those who do get sick.
Vaccine misinformation has put millions of people unnecessarily at risk, but it is not too late to fix that.
Get boosted, wear a mask, and stay strong. Together, we’ll make it.