The Weather Outside is Frightful and That’s Just the Half of It

Lisa Suennen
I really miss waiters.
I was recently talking, via the mixed blessing of Zoom, with the very awesome members of a women’s group to which I belong.
Our full group of about 35 meets once a year. Normally, we do so in person, at a spa, where food is brought to us by actual waiters.
Remember waiters? Man, I miss waiters.
But despite talking via Zoom and definitely not in the company of waiters, the plan for this year was still the same as always: each of us in virtual attendance would get 15-20 minutes to talk about whatever we want. It’s wonderful.
You can solicit advice. You can ask for silence. You can open up about your deepest moments of loss and sadness or your small and large victories. You can brag about your family or complain about them. You can share your work challenges or talk about your excitement about opportunities ahead. And you can whine, bitch, moan and lament to your heart’s content and get unqualified and loving support from the best pit crew ever.
When it was my turn to pour my guts out, I tried to describe the silver linings of the current world order (or at least my slice of it). There are many, and I reminded myself of them this past Thanksgiving weekend. I have much for which to be thankful.
But I also ended up unloading on my friends about all of the things that Just. Totally. Suck.
Normally, I’m not one to unload a double-barreled shotgun of crap on other people. But I was struck by the tidal wave of positive reinforcement I received while wallowing in suckage, and particularly the sense that this suckativity is shared at a visceral level by so many who look like they have their acts totally together. It was kind of cathartic for me, and apparently for others in the group, too.
I left that Zoom call encouraged to write about it, because I realized these are shared experiences, not my own personal hell.
So lucky you, welcome to my “Life Sucks the Big One” blog post.
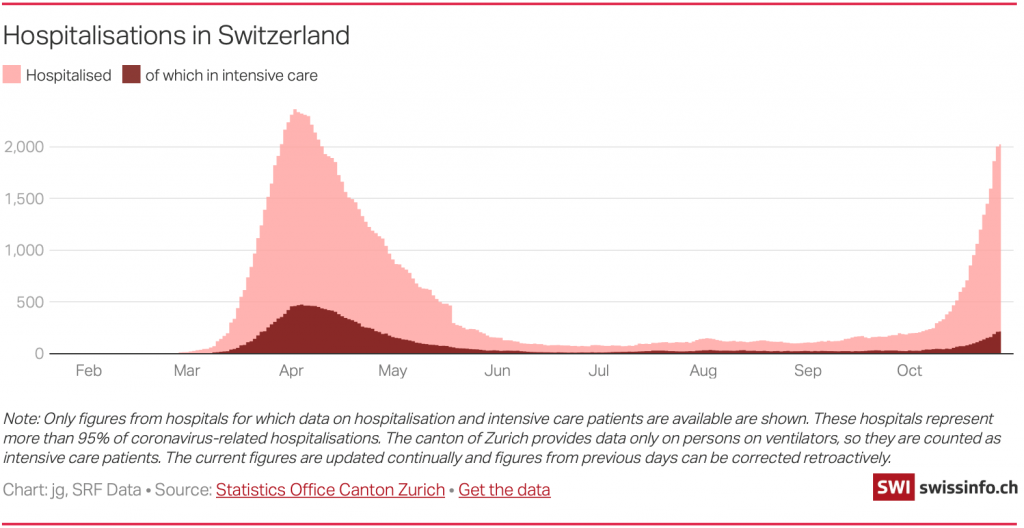
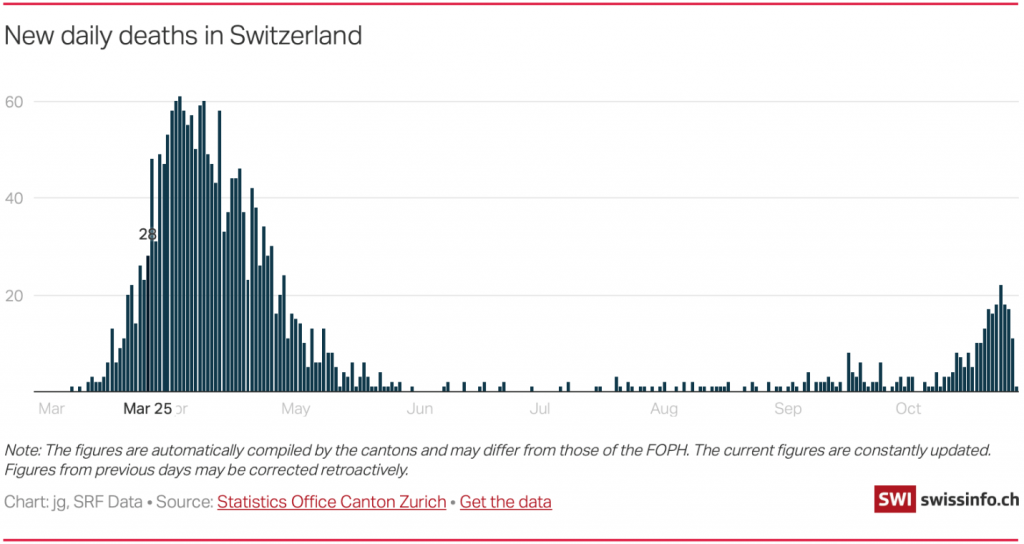
We all know the toll this pandemic has taken on our families, friends and selves. The number of deaths or terrible illnesses experienced is beyond words.
And yet, for those of us fortunate enough to have avoided the virus, there is tremendous guilt. Complaining too much about how we are feeling, mentally and emotionally, during this shitstorm of a year feels petty and wrong.
You don’t have to look around long to see extreme suffering of others.
And yet, the seemingly small miseries of those of us with COVID survivor’s guilt do exist. They are real (if not spectacular — congrats if you get that joke).
The mental health of many is taking a toll and I’ll admit to being one of those doling out quarters at this particular toll bridge. I have definitely been down-beat more than usual. I can cry at the slightest thing. Sentimental toilet paper commercial? Here come the tears. I run out of ice cream, here come the water works. God help me if I read a story in the newspaper that reminds me how much crap is going on in the real world – it makes me try to burrow under the couch (so THAT’s where all the dog toys are).
The only upside is that I gave up makeup sometime in April and thus I am saving money on all the mascara that would otherwise now be streaming down my cheeks.
I have a constant sense of fear and paranoia about getting sick. I’m annoyed that a few of my friends have exerted some peer pressure about getting together in ways that just don’t seem optimal under the COVID circumstances.
I feel bad saying No, but would feel stupid saying Yes. Few would mistake me for an introvert, yet I am doing my best impression of one and it is getting more and more natural. Sometimes I wonder if I’m turning into a hermit. That also sucks.
I miss traveling and seeing people. It is scary to think that the huge network I have built over a lifetime is somehow moving ahead without me. When I’m being sane, which occurs every other Thursday from 7:32 am to 7:36 am (now the best time to reach me) I realize that there is so little going on out there that my fear of being left behind is unlikely to translate in reality. Even so, it gnaws at me, driving me at moments into of a crazy kind of FOMO. For those who don’t use this acronym several times a day, Fear of Missing Out is an occupational hazard for venture capitalists and entrepreneurs in the best of times.
Turns out, I’m not the only one feeling the FOMO dialed up to 11. I was fascinated to learn that this is also at the top of the list of worries for so many of my women’s group friends. COVID stress and anxiety is apparently triggering an epidemic level of insecurity and low self-esteem that would be wholly unexpected among this crew of accomplished over-achievers.
One of the things I worry about (and worry about how I’m worrying about it) is how I have lost, at least for now, some of the silly but real ways I used to define myself in the world.
Those who know me even a little bit know how much I love shoes. Yet I haven’t bought a pair of shoes in about 8 months. This has to be some kind of personal record. I suspect that any economic woes being experienced by Manolo Blahnik and the Nordstrom shoe department are directly traceable to me and my absence.
Furthermore, I always ran around in the world with elaborately painted toenails. Again, hardly a life crisis to have naked toenails when so many people I know are truly suffering, but it was a mode of accessorizing that kicked off a lot of fun conversations and a means of self-expression that I have really enjoyed for well over a decade.
That’s actually the crux of this – the lack of access to things that “bring me joy,” as Marie Kondo would say. If a person is the sum total of their triumphs and tribulations (and toes), and there are few triumphs (because they are hard to achieve when locked up like Rapunzel after a big haircut), and too many tribulations – then you start to feel like a pale version of your former self. Certainly, it’s hard to feel like you’re at the top of your game.
And, speaking of games, up until March I also played squash 2-3 times a week for most of the last 16+ years; that is, alas, also gone for now. Not only does squash make for good aerobic exercise, it used to be the primary way I removed stress from my system. Smashing things repeatedly while swearing, it turns out, is excellent therapy.
My gym in Northern California is remarkably still open. They keep calling me to come back. Part of me wants to go back. But given that what I would do there is lock myself into a small, fully enclosed room with little circulating air and with another sweaty person expelling spit through aggressive swearing, I’m thinking…probably not such a great idea.
Alas, leisurely walks through the park just don’t cut it for my fitness routine. It turns out that if you stomp aggressively down the street while swearing, people stare and dial 911.
My coping skills, as a result of my sloth-like fitness routine, are less than stellar. On the plus side, my over-reaction time is dropping so fast I could win some sort of panic contest. Everything that goes wrong feels like a disaster. Spilling water from a glass could trigger an international incident.
Like everyone else in America trying to soothe rattled nerves, we got a puppy. The little critter is cute as can be and needs a ton of attention; so, naturally, any extra time available is time I spend feeling guilty about how little time I am spending with the cat. Look, I’m Jewish, so anxiety comes with the bloodline, but this is getting ridiculous.
So why am I telling you all this? It is not for sympathy. It is for connection and so we can all share a little self-validation.
The feelings of guilt, insecurity, isolation, anxiety, loss of self-expression – they seem to be universal constants right now. Most of us are feeling stressed, anxious, a little lonely, a little lost and very stir-crazy. The idea that we may have months or even another year of this to go is daunting. We have gone from talking about testing 103% of the time to talking about vaccination timelines morning, noon and night. Yes, there was a momentary election conversation interlude (thank God that’s over with), but otherwise it’s all COVID all the time.
For many people it’s really tough to share feelings, no matter what the circumstances. It is especially tough when those feelings seem shallow as compared to the true depths of despair that so many families have faced. But as one of my friends pointed out, misery doesn’t have to be a zero-sum game – we are all entitled to our feelings and fears and to having those validated. In fact, if we don’t let the feelings out, we are going to start seeing people spontaneously combust in the grocery store.
Some of us are self-medicating in ways that we normally never would. By the way, if you’re at the grocery store buying chocolate and can’t find any, it’s because I ate it all.
But seriously, alcohol and drug consumption is booming (Nielsen reported a 54 percent year over year increase in alcohol sales during the initial pandemic surge in mid-March). That is terrifying considering how that alcohol consumption had been steadily rising for 25 years, even before the pandemic. We really don’t know what damage we will all be left with psychologically, physically, and culturally after the pandemic passes.
So, again, it’s essential to find ways to express your feelings, to feel validated for having them and to know you are not alone. We may have a country that is quite divided, but bottom line, we are actually all in this together. Never has it been clearer that we are as connected as the bones in that old song – our knee bones are connected to our leg bones and so on. There is no getting around it.
So, here’s my request: ask a friend or acquaintance how they are doing and really hear them out. Listen to their litany of woe and do not judge. Validate. One person’s little problems are another person’s crisis. Your job is to empathize and support. Acknowledge. Be there. Be attentive. Err on the side of loving kindness. And when that is done, be kind to yourself and seek the reciprocity you deserve. We will get past this if we help each other through.